IR-202308-1: Fatality from nitrous oxide-induced hypoxia
| Outcome | Fatality |
|---|---|
| Age of victim(s) | 29 |
| Date | August 2023 |
| Location | Subject's home, Northwestern USA |
| Involved kinks | Breath play, Inhalants, Intoxication play, Nitrous oxide |
| Number of people present | 1 |
| Identifier | IR-202308-1 |
| Published | 2025-01-17 |
| Last updated | 2025-01-17 |
The subject of this report is a 29-year-old who died while playing alone at home with nitrous oxide in a semi-closed rebreathing circuit. Although the subject was considered to be an experienced practitioner of breath play, their fail-safe system did not function as intended, resulting in the fatal event. The evidence suggests that the subject was continuously exposed to a hypoxic gas mixture from the uninterrupted flow of nitrous oxide into the circuit and lost consciousness. From our analysis, we believe that a subtle operational design flaw combined with the direct connection of a large supply of nitrous oxide to the breathing circuit led to death occurring before oxygen could be restored.
Environment
The fatal incident occurred in the subject’s home. The subject lived alone in a detached 1-bedroom unit. The subject’s body was found on a couch in their living space with a gas mask attached to their face, which was connected to a large nitrous oxide tank through a self-built breathing circuit. They were wearing only underwear and were lying under a comforter with their hands clasped around the nitrous oxide control valve of the breathing circuit. A vibrator was near the subject but did not appear to have been used.
Individuals referenced
- (S) - The subject of this incident report. According to multiple friends, (S) was described as very experienced with kink and breath play in particular. The subject was aware of the risks of solo breath play, had experienced near-miss incidents involving nitrous and breath control, and attempted to mitigate the risks in the design of the breathing circuit used.
- (A) - Friend of (S) who lived near them and had a key to their unit.
- (B) - Friend of (S) who lived in the same area and was a regular play partner of (S).
- (C) - Friend of (S) who had discussed a near-miss incident involving (S) at an event.
Timeline
Preceding events
Friends of (S) witnessed events and circumstances in the months leading up to the fatal incident that raised concerns about (S)’s safety relating to their practice of breath play. However, these previous incidents occurred amongst different individuals and groups of friends, so no individual had a comprehensive perspective of the escalation in the intensity and risk that (S) may have been taking.
Several months prior to the fatal incident, one friend (A) observed (S) disposing of a large trash bag full of empty whipped cream chargers (each of which contained a small amount of food-grade nitrous oxide) at their shared garbage bin. (A) confronted (S) about the quantity of use, and (S) reported they were going through a stressful time at work. After this confrontation, (A) did not witness (S) having whipped cream chargers again, speculating that (S) started disposing of them elsewhere to conceal their use, though this could not be confirmed.
Sometime after this, (S) was introduced to the availability of larger containers of nitrous oxide. (S) expressed interest in acquiring a larger tank for cost efficiency and ease of use. Reportedly, the subject was aware of the potential risks of solo breath play and knew that using nitrous oxide in a closed circuit was dangerous.
Several weeks prior to the fatal incident, the subject was the subject in a bondage and breath play scene at an event in which nitrous oxide was intermittently administered into a closed circuit. According to a friend (C) who witnessed it, people expressed to (S) their concerns about the dangers observed during the scene. However, in discussions afterwards (S) was dismissive of them.
In another instance prior to the fatal incident, (S) experienced a near-miss which they discussed with another friend (B). (S) was playing alone with a rebreather bag and nitrous oxide, lost consciousness, and awoke on the floor with the bag in their hand and no recollection of the preceding moments. Upon hearing this, (B) became concerned and advised (S) to not do breath play alone.
Fatal incident
(S) had returned home from a work trip abroad on the day of the fatal incident. They had plans to meet with (B) in the early evening of the following day. When (B) arrived the next day, (S) did not answer their door. (B) looked inside the window of (S)’s unit and could see that (S) was on the couch and not moving. (B) contacted (A) who lived in another building on the property and had a key to (S)’s unit.
Upon entering the home, (A) and (B) found (S) laying unresponsive on the couch wearing a gas mask connected to a large cylinder of nitrous oxide with their hand clenched around a valve. The carpet around the nitrous tank was noted to be damp, presumably from condensation resulting from the complete continuous decompression of the tank. Based on (A)'s experience in emergency rescue, (S)’s temperature, signs of blood vessel collapse in the feet, they estimated that (S) died between 23:00 and 02:00 the previous evening. (A) called emergency services and officers and medical examiners arrived shortly thereafter.
Incident analysis
Cause of death
Based on the circumstances in which (S) was found, it is believed that (S) died from hypoxia due to continuous flow of nitrous oxide into their breathing apparatus.
Attempts to mitigate risk
(S) was known to be very experienced and informed about the risks of breath play. They were reportedly mechanically inclined, and designed a breathing circuit (Figure 1) which they believed to be fail-safe based upon two key features:
- A control valve which was held closed by a spring and would only allow the introduction of nitrous oxide into the circuit when manually held open by pulling a trigger.
- A one-way inspiratory demand valve on the gas mask, which was designed to automatically open and passively allow room air to enter the circuit during inspiration. Importantly, this valve cannot open unless the internal circuit becomes negatively pressurized from an inspiratory effort.
It is assumed that (S) believed this design was fail-safe because if consciousness was lost, their hand would release the control valve, causing the flow of nitrous oxide to cease and allowing the flow of fresh oxygen through the inspiratory inlet valve of the gas mask.
-
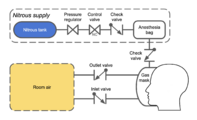
Figure 1: Schematic of the breathing circuit used during the incident. Nitrous is colored blue, room air is colored yellow.
-
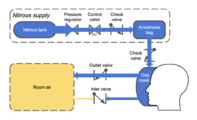
Figure 2: Conditions where the control valve is open. Arrow thicknesses represent relative pressures. Nitrous flows from the tank through the anesthesia bag and pressurizes the gas mask, preventing the inlet valve from opening.
-
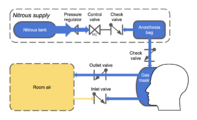
Figure 3: Control valve closed. Nitrous is only supplied to the gas mask by the anesthesia bag. The inlet valve remains closed while there is sufficient nitrous remaining to pressurize the gas mask.
-
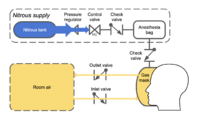
Figure 4: Nitrous in anesthesia bag exhausted. The wearer's lungs generate enough pressure to open the inlet valve, allowing oxygenated room air into the gas mask. This represents the intended fail-safe condition which was not effective in this incident.
-
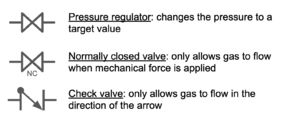
Figure legend: A reference for the symbols used in the figures of this report.
.png)
.png)
.png)
.png)

Unanticipated conditions
Hypoxia-induced posturing

Under normal circumstances, the brain constantly transmits inhibitory signals through the spinal cord which keep the muscles of the body relaxed when movement is not evoked. When the brain loses consciousness due to hypoxia (or otherwise becomes disconnected from the body), the lack of inhibitory input causes many muscles of the body to continuously contract in a predictable pattern called posturing. One important feature of posturing is that the hands tend to tightly clench. The contractions from posturing also don’t tend to release until normal brain connectivity is restored (i.e. oxygen is delivered), meaning that the posturing position can persist through brain death into rigor mortis.
Large supply of nitrous oxide
There was an adequate supply of nitrous oxide from the tank to maintain continuous flow into the circuit for several minutes. The large volume tank was selected to optimize for cost, but increased the risk by increasing the amount of time that the breathing circuit could be pressurized with no oxygen.
Fatal combination of factors
Based on the evidence, (S)'s death likely resulted from this sequence of events:
- (S) held the trigger valve open to introduce nitrous oxide into the breathing circuit.
- (S) lost consciousness from hypoxia which caused their body to assume a posturing position. In this state their hand clenched and held the trigger valve open, resulting in continued flow of nitrous oxide even after they lost consciousness.
- Because nitrous oxide continued to flow, the breathing circuit maintained positive pressurization as shown in Figure 2. This prevented the expected fail-safe one-way inlet valve on the gas mask from opening, so oxygen-rich room air was unable to enter the circuit.
- There was enough nitrous oxide in the tank for at least several minutes of uninterrupted flow, leading to total respiratory arrest from continued brain injury. Past this point, (S)’s body ceased attempting to breathe and brain death rapidly followed.
Discussion
False confidence
(S) was highly experienced with kink and breath play. This likely gave (S) a sense of confidence that they understood the dangers of solo breath play and that they could design a breathing circuit which would be fail-safe. It is assumed that (S) was not aware of the posturing phenomenon, causing the incorrect assumption that if consciousness was lost their hand would release the trigger valve and restore normal air flow.
Their headspace and the casualness of the scene may have also impacted their risk assessment. This was not a complex configuration involving bondage or many pieces of gear. Evidence suggests that this incident was a casual intoxication-enhanced masturbation session to relax after a long work trip using only the gas mask and a vibrator.
While knowledge and experience are powerful assets to facilitate the safe practice of kinks, this incident represents an example of how a false sense of confidence from incomplete knowledge can pose grave danger. When the desire to pursue increasing intensity causes escalation of risk taking behavior, the danger is tragically amplified if the knowledge of possible risks is incomplete. The editors of RACKWiki believe this incident is an important reminder to the kink community that even experienced practitioners can become victims of serious unintentional harm.
Pattern of behavior
There were warning signs present that (S)’s behavior relating to breath play and nitrous oxide use was escalating dangerously beyond safe practices leading up to the fatal incident. In the month leading up to their death, (S) had a distressing experience during one incident at an event, and uncontrollably lost consciousness and fell to the floor from self-asphyxiation in another. (S) described both of these experiences as negative and scary, yet neither caused (S) to change their risky behavior. Thus, even if they avoided the fatal outcome in this incident, (S) would still have been at very high risk of a fatal incident unless a holistic intervention succeeded.
This assessment does not attribute ultimate responsibility to the people around (S). No individual had a complete picture, and no individual can completely control another person’s behavior. An intervention may not have changed (S)’s behavior, but in reflecting on the incident, several of their friends wished they had tried harder.
Continuing consequences
The friends and family of (S) are still dealing with the aftermath of this incident more than a year since it happened. Without written instructions from (S) on how they wanted their possessions taken care of, the friends had to decide on the numerous items that the family yielded to their care. Many of these are pieces of kink gear that are intimately tied to (S)'s identity, complicating decision making among their friends. More than a year later, the majority of the items have remained in storage despite friends agreeing on who would take ownership due to the emotional trauma from revisiting this painful event.
Risk mitigation analysis
Solo breath play is a dangerous practice which should never be encouraged. It is possible that alteration of any of the following conditions may have prevented the fatal outcome of this incident, but not all of them could have been possible:
- Having a play partner present during play to ensure oxygen can be restored even after consciousness is lost.
- The use of a breathing circuit which cannot remain attached to the face without conscious effort.
- The use of a triggering mechanism for nitrous oxide that cannot be held open by a clenched hand.
- The use of a smaller tank of nitrous oxide which would be unable to maintain flow significantly past the point of loss of consciousness.
- Recognition and intervention in response to signs of escalating risky behavior in the months leading up to the incident.
Recommendations
- Although complete risk mitigation is impossible for solo breath play, there are steps that can be taken to significantly mitigate risk in most circumstances. It is unfeasible to account for every possible factor that could lead to a fatal incident if consciousness is lost. A second person in the scene who is able to respond to off-nominal conditions greatly increases survivability.
- If you see someone engaging in escalating dangerous behavior, talk to them and the people around them. An intervention is not guaranteed to succeed, but a lack of intervention is guaranteed to fail.
- Prepare a will and/or written instructions. In most jurisdictions your estate is left to your family if there is no will. Leave instructions on how to dispose of your possessions to ease the burden on friends and family.
Report authorship and information sources
This report is based on information from a primary source who submitted an incident report form (individual A), and 2 additional secondary sources (individuals B and C). The sources were interviewed by RACKWiki staff, who independently corroborated their accounts across sources and using publicly available information.
The report was written by 2 primary authors (Yupcake and Psynapse) and reviewed by 5 additional members of the RACKWiki editorial staff (Rage, XcamcassX, and three reviewers who wish to remain anonymous). Additionally, all information sources were given the opportunity to review the report and provide feedback prior to publication.
If you have questions, comments, or feedback, please use this report's discussion page or reach out to the RACKWiki staff using our contact form.
Revision history
| Date | Summary |
|---|---|
| 2025-01-17 | Initial publication |
| 2026-07-23 | Revised Discussion based on feedback |